
The headlines shout about the growing death toll from coronavirus, but there is less focus on the link between mortality and population density. That’s surprising because the link appears to be strong – certainly in the US and EU.
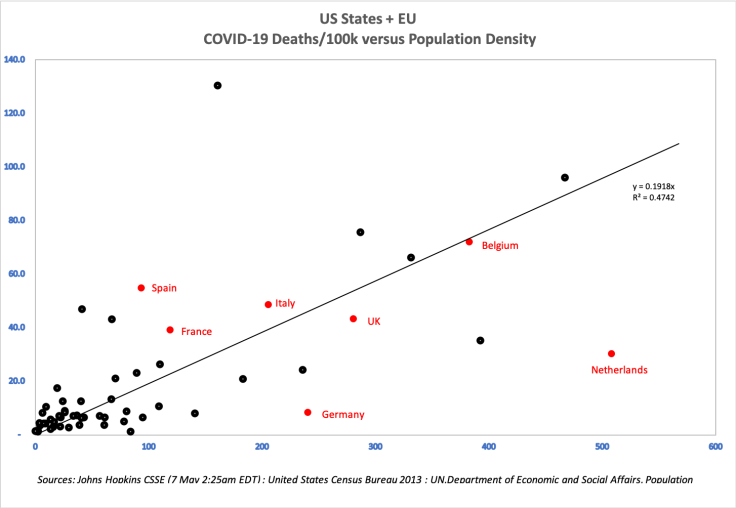
Check out this chart of mortality as of 7 May 2020 in the 50 states of the USA plotted against that state’s population density measured in people per square kilometre.

The relationship is statistically very significant (t-statistic above 9) and, although there are a few outliers (New York for instance) and there is a lot of unexplained variance, an r-squared of near 50% is pretty high in social science.
Intuitively the relationship makes sense: we’d expect a higher spread of a disease in regions that are densely, rather than sparsely populated. It’s also consistent with the lessons of historic pandemics. For instance, it is well documented that mortality during the 14th century Black Death was higher in cities than in rural locations.
Although international mortality comparisons are fraught with difficulty arising both from differences in methodology (do you have to die of Covid-19 or merely with it? Do you have to die in hospital or does anywhere count?) figures from the culturally and legally more homogeneous USA should avoid many of these problems.
What explains the rest of the variance? A whole slew of factors, no doubt: the degree of connectedness to the rest of the world (which might explain New York); the timing of the outbreak; the timing and strictness of any lockdown; the ability of the state’s health system to cope; even the ethnic make-up of the state’s population.
This is certainly the case if the findings published today in the UK – that BAME patients are doubly likely to die of the disease than white people even adjusted for differences in income and health – are replicated in the USA.
And what of Europe?
As I mentioned, there are difficulties comparing the mortality in different countries, but, overall, the picture in the EU seems to consistent with the USA. See the graph below where European data is added. Clearly, Germany and the Netherlands are outliers (methodology or policy? I can’t say), but many of the other nations are bang in line.
What does this all matter?
Probably not much right now as we are in the middle of the crisis. But when the dust settles and the inevitable public inquiries start, I expect we’ll see much more focus on factors like this from governments – both at regional and national level – looking to avoid blame.
Me? I can’t wait.
****************
Postscript
A couple of readers have pointed out that many Asian countries with much higher population densities than the USA or EU (notably Hong Kong, Taiwan and Singapore) have had very different mortality rates. That is of course entirely true and is testament to a radically different policy approach: very strict early lockdown combined with stringent trace and contact. This approach was developed in the region after the lessons of SARS – lessons that were lost on western governments.
The one puzzling exception in all this is Japan which has a population density of 336 people per square kilometre, low mortality (590 as of 7/May/20, or 0.47 deaths/100k) and an approach to lockdown that seems more in line with the EU than Hong Kong. All the bowing? Who knows. I’m sure we’ll find out in the years ahead when the doctorates get written.
*****************
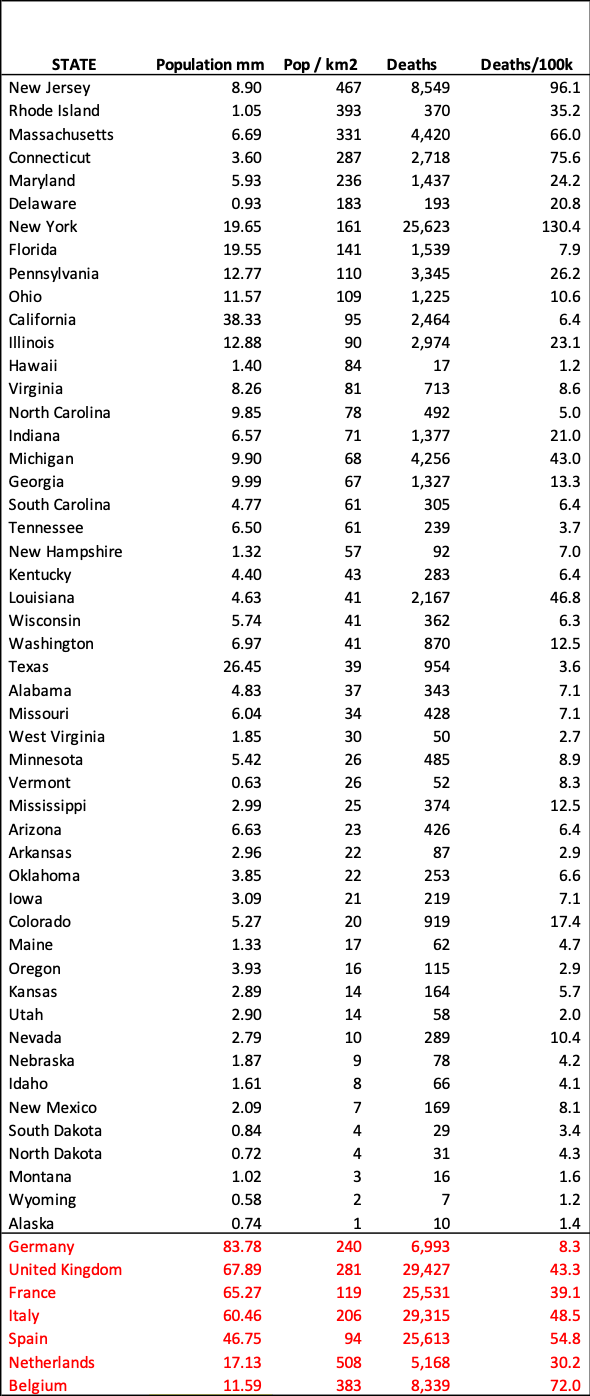
Data table for the graphs case you are interested.

May 7, 2020 at 12:21 pm
Thank you , interesting article . How come Japan which has Tokyo , one of the , if not the most densely populated cities in the world , has such a low death rate ? is it purely down to a culture of wearing masks and bowing ?
LikeLike
May 7, 2020 at 12:24 pm
I don’t know. Personally, I suspect it isn’t masks, but some mix of timing, policy and possibly genetics. I’m sure PhDs will be written on this for years to come.
LikeLike
May 7, 2020 at 12:26 pm
I don’t know. Probably not masks (not sure they do much) but a mix of timing, public health policy and -possibly – genetics.
LikeLike